
Any tube intended for the stomach, yet is inadvertently placed or subsequently dislodged to anywhere except the stomach, may result in a life-threatening condition. This is because fluids that enter the lung may lead to an infection commonly referred to as pneumonia. This is especially critical for patients, such as neonates, as they are purposely positioned prone or supine during feeding. This may ultimately lead to unexpected or undesired backflow to a lung from the esophagus.
The use of pH testing, when appropriate, is validated nationally by organizations for nutrition, patient safety, and emergency care. These apply for caring of neonates, infants, and adults. And pH testing provides best-practice evidence-based nursing care, especially over auscultation (whoosh test). Studies confirm patients benefit from reduced exposure to radiation, delays in feeding, medicating, or irrigating. And pH testing even reduces costs over X-rays. All RightSpot® pH Indicators are FDA cleared/CLIA Waived Class 1 devices.
For additional context, review our Clinical Evidence and the latest Instructions for Use.
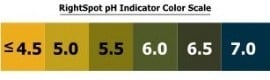
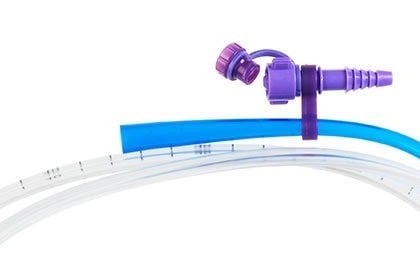
RightSpotpH® ENFit® Indicators fit ENFit® system tubes and ENFit-compatible syringes. RightSpotpH® Small Bore Indicators fit legacy enteral syringes and legacy tubes 10 Fr or smaller. RightSpotpH® Indicators fit luer lock syringes and tubes larger than 10 Fr. All include an on-device pH reference scale from ≤4.5 to 7+ in 0.5 increments.
No. The indicators are designed to work with nearly all manufacturers’ brands and sizes of NG/OG feeding, suction, or lavage tubes and enteral syringes. If you use Vygon Nutrisafe 2® compatible tubes, contact us for adapter guidance.
Absolutely. They are the number one selling brand of in-device pH Indicators for use with ENFit®. However, we are continuing to support the legacy tubes and syringes for the time being.
No. RightSpotpH® Indicators and the syringe used to withdraw aspirate are single-use items. Remove and dispose of the indicator and syringe together per facility policy.
Before aspiration, purge the tube with air to clear residual fluid: neonates 3-5 mL, pediatric patients 5-10 mL, and adults 10 mL or more. If aspirate is still not obtained, position the patient on the left side (if tolerated) for 10-15 minutes and reattempt. If still unsuccessful, follow facility protocol.
References: NHS Resource Set Initial Placement for Nasogastric and Orogastric Tubes (July 2016); Journal of Neonatology/Perinatology NICU Journal study (Fall 2015).
The need for these is at the discretion of the Laboratory. The unique packaging of all RightSpotpH® Indicators protects each device from light, air and humidity. Our devices also support extended outdates of up to 2 years unopened and a wide temperature storage range of -40°F to 125°F. Incidentally, most other pH papers and pH strips require revalidation thirty days after opening and temperature storage at 85°F or below.
Only enough to change the color of the pH indicator. Once you see the color change, stop pulling aspirate. For all RightSpotpH® Indicators it is at most 0.5 mL. Do remember to draw up and purge air through the line before aspirating. Consider for neonates 3-5 mL, for pediatric patients 5-10 mL and for adults 10 mL or more. The goal is to completely purge the tube of any residual fluid to allow for aspiration from the tube tip.
Device-specific ENFit note: The 0.5 mL Small Bore amount applies to RSSB001 workflows, not RSEN001. The RightSpotpH® ENFit Indicator (RSEN001) requires 3-5 mL because of the device’s increased prime volume. The air is immediately aspirated back out during the workflow. Follow the product IFU and your facility protocol.
Yes, the device may be used in a homecare environment if the user has been properly trained. However, Indicators are not yet available for sale directly to the public. Because pH testing is a laboratory test, if an individual is to be utilizing it, they need to be trained and provided the device. Some hospitals do this to alleviate the need for patients to return through the Emergency Department simply to have the tube verified, adjusted, or reinserted. Requirements to use this Class 1 device include a high school diploma or equivalent and documented training by the hospital provider. Please consult with your specific provider for details.
Yes. But importantly one must time the pH testing around the dosing of these medications. For example, oral PPI or H2 Blockers require 2 or more hours after dosage to adequately metabolize the medication below the threshold of ≤5.0 or ≤5.5. Intravenous (IV) PPI or H2 Blockers, such as Protonix® or Nexium® IV, require 4 or more hours after completion of dosage to adequately metabolize the medication below the threshold of ≤5.0 or ≤5.5.
Tube position can change after events such as vomiting, transfers, replacement, coughing, or patient movement. Frequency of re-checks should follow facility protocol and patient-specific risk factors.
It depends. If aspirate appears as digested/coagulated blood (coffee-ground appearance), use may be appropriate. If aspirate is bright red, do not proceed and follow facility escalation protocol.
Yes. The RightSpotpH® Indicator was initially designed by and for ED usage after two sentinel events occurred, each resulting in charcoal being tragically administered to the lung. Thus either the RightSpotpH® Indicator or RightSpotpH® ENFit® Indicator will fit large bore tubes >10 Fr. In addition, many Salem® Sumps now come with a reusable repositionable ENFit® connector for use with ENFit® enabled syringes and the RightSpotpH® ENFit® Indicator. Ask your Salem Sump provider for more information.

For device-specific workflow, review the Instructions for Use.
Before administering fluids or suction, correct tube-tip placement should be confirmed. pH testing can provide immediate bedside information and may reduce delays while waiting for imaging in appropriate use cases.
Lung tissue is vulnerable to injury from unintended suctioning. Immediate confirmation steps can reduce risk before treatment proceeds.
The ENA Clinical Practice Guidelines 2015 do not recommend auscultation for confirming tube placement. Their recommendation is to use pH testing, if appropriate, or X-ray. All RightSpotpH® Indicators are designed for tip position verification of tubes intended to end in the stomach. The devices incorporate a novel closed system protecting the clinician, patient, and environment from exposure to bodily fluids, which may contain blood. And each single-use pH testing device provides for purging the tube of prior fluids, quick accurate specimen collection, in-device on-board testing, validated result determination and, finally, proper disposal per hospital protocol.
Studies confirm reduced patient radiation, delays in usage, and lower costs over X-rays. Reference: ENA Gastric Tube Placement Verification guideline (2015).
Yes. Our CPT Code is 83986QW and the reimbursement is $4.80 or more, depending on the payer. See your Lab Manager for details.